Cambridgeshire and Peterborough Child Death Overview Panel Protocol
Table of Contents
Glossary
| Joint agency response (JAR) | A coordinated multi-agency response (on-call health professional, police investigator, duty social worker). The full process for a Joint Agency Response is set out in the SUDI/C Guidelines. |
| Child safeguarding practice review (CSPR) | An independent review into a case where a child has been seriously harmed or has died and abuse or neglect is known or suspected. The aim of a CSPR is to establish any lessons learnt from the case and to identify how these have, or will be, acted upon and lead to sustainable improvements to practice and the prevention of death, serious injury or harm to children and young people. |
| eCDOP | Developed to support the CDR case management and reporting process. The eCDOP system uses the statutory forms and process from the Working Together 2018 guidance and assists safeguarding teams to ensure compliance. |
| Child death overview panel (CDOP) | Child Death Overview Panels (CDOPs) were enacted as a statutory requirement of Working Together 2010. The purpose of the CDOP is to ensure that when a child under the age of 18 dies there is a comprehensive and independent review of the circumstances. |
| National Child Mortality Database (NCMD) | An NHS-funded programme delivered by the University of Bristol that gathers information on all children who die in England, so that they can improve and save children’s lives in the future. |
| Neonatal | Neonatal means newborn, or the first 28 days of life |
| Child | A person under 18 years of age. For the avoidance of doubt, it does not include stillbirths, late foetal loss, or terminations of pregnancy (of any gestation) carried out within the law. • Stillbirth: baby born without signs of life after 24 weeks gestation • Late foetal loss: where a pregnancy ends without signs of life before 24 weeks gestation. Cases where there is a live birth after a planned termination of pregnancy carried out within the law are not subject to a child death review. |
| Child Death Review Partners | Defined in section 16Q of the Children Act 2004 and means, in relation to a local authority area in England, the local authority and any ICB for an area any part of which falls within the local authority area. |
| Coroner’s inquest | Inquests are legal inquiries into the cause and circumstances of a death, and are limited, fact-finding inquiries; a Coroner will consider both oral and written evidence during the course of an inquest. |
| Perinatal Mortality Review Toolkit (PMRT) | The PMRT is a web-based tool that is designed to support a standardised review of care of perinatal deaths in neonatal units from 22+0 weeks gestation to 28 days after birth. It is also available to support the review of post-neonatal deaths where the baby dies in a neonatal unit after 28 days but has never left hospital following birth. |
1. An introduction to CDOP
The CDOP is set up by the child death review partners, Cambridgeshire and Peterborough Local Authorities and Cambridgeshire and Peterborough Integrated Care Board. The CDOP ensures that agencies are compliant with statutory guidance Working Together to Safeguard Children: December 2023[1] and the Child Death Review: Statutory and Operational Guidance 2018[2].
The CDOP protocol is based upon both statutory guidances and should be read in conjunction with them.
The panel undertakes two inter-related processes to understand and review all child deaths, these are:
- To collect and analyse information surrounding the death of all children under 18 years old in Cambridgeshire and Peterborough with a view to achieve:
- Reduction in numbers of child deaths
- Prevention of accidents to children
- Identification of, and understanding of patterns of childhood death
- Support for parents and families of deceased children
- Improvement in interagency practice
- Education of public and professionals working with children
- Highlighting any matters of concern
- Identifying the need for a child safeguarding practice review (CSPR)
- To oversee the process of conducting a joint agency response (JAR) with a group of key professionals to enquire into and evaluate the unexpected death of any child.
Either of these processes may identify abuse or neglect as a factor in the death and if so, this would be reported to the Safeguarding Partnership Board for consideration of a rapid review, with a decision then being made as to whether it meets the criteria for a CSPR.
The child death review process involves the following:
Notification
Professionals in all agencies have a responsibility to notify the relevant CDOP where the child lived, of the death of any child of which they become aware via the eCDOP system. They also have a duty to share information for the purposes of reviewing the child’s death, and to participate in local review arrangements when they have been involved with the child or family.
Information gathering
- The CDOP manager is responsible for gathering agency reports relevant to the child who has died. Requests for agency reports will be made using the eCDOP system within 5 working days of confirmation that the child is known to agencies but will usually be sent the same day where possible.
- Agency responses should include a full report or nil return where they were not involved with the child or family.
- Prompts will be automatically generated via the eCDOP system at two, four and eight weeks from the initial request. If an agency has not responded within 10 working days of the third prompt, this will be escalated to the Designated Doctor for Child Death Review and the CDOP chair of the area in which the organisation sits.
Preparation for review
- Once all agency returns have been completed, the CDOP manager will summarise the key events in the child’s life, including their medical history and family circumstances. This will be presented in the form of a timeline, with dates and times where available.
- Once the summary timeline has been completed it will be assigned to the next panel meeting via the eCDOP system. This will make the child death analysis form available to all invited panel members when securely logged in to eCDOP, no less than 1 week prior to the panel meeting.
During the review
- All CDOP members will commit to reading the CDOP case papers in advance of the meeting to avoid delay in coming to a determination for each case.
- The Chair, Vice Chair or other nominated person will present the key factors surrounding the child’s life and circumstances leading to their death. The timeline should be followed to allow gaps or incongruous events to be visible.
- The panel should endeavour to come to an agreement regarding the category of death. Where consensus cannot be reached, it is preferable to seek further information and, if necessary, ask the opinion of other CDOPs via secure communication channels rather than resorting to a vote. This approach also applies to the question regarding the presence of modifiable factors.
- The panel may differ in opinion from a Coroner’s inquest, or other statutory investigations.
- CDOP may make recommendations to the Safeguarding Partnership Board or other relevant bodies so that action can be taken to prevent future such deaths where possible.
- Where a suspicion arises that neglect or abuse may have been a factor in the child’s death, CDOP must refer the case to the Safeguarding Partnership Board for consideration of local learning review and/or report to national panel.
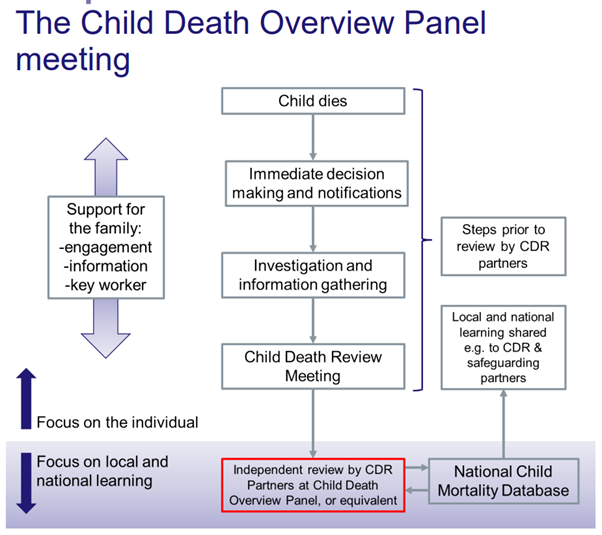
See appendix one for the CDOP review process flowchart.
2. Key functions of the CDOP
The CDOP must ensure, in conjunction with the relevant Coroners procedures and protocols it complies with Chapter 5 of Working Together to Safeguard Children, March 2018 and Child Death Review: Statutory and Operational Guidance, 2018 to enquire into and review all children’s deaths in the area.
The CDOP will collect a minimum data set as required by the National Child Mortality Database and submit via eCDOP for national data collection.
Where relevant and appropriate, the CDOP will seek further information from professionals and family members should they wish to contribute to the process.
The CDOP membership will meet quarterly to review and evaluate anonymous data on all child deaths, with a focus on effective interagency working.
Deaths of neonates who do not leave hospital during their lifetime are considered separately by Perinatal Mortality Review Toolkit (PMRT) with members including representatives of Midwifery, Obstetrics and Neonatology. This panel is chaired by the Neonatal Mortality Lead for the relevant hospital who will escalate any concerns to the CDOP Chair.
The panel will oversee professionals’ responses to an unexpected death by reviewing the reports as part of the JAR process, recording this discussion, and enabling feedback to be given on professionals’ roles.
Cases involving a criminal investigation will usually not be reviewed before the conclusion of proceedings.
Where relevant, the CDOP will provide information to a professional working with the deceased family, so they can convey this information in a sensitive and timely manner to them.
The CDOP will monitor whether support and appropriate assessment services are offered to families of children who have died.
The CDOP will identify any public health issues and consider with the Director(s) of Public Health, how best to address these and their implications, for both the provision of services and for training purposes.
The CDOP will report annually to Cambridgeshire and Peterborough Safeguarding Partnership Board, with relevant and anonymous information. The CDOP will present recommendations to improve policy, professional practice, and inter-agency working to safeguard and promote the welfare of children by reducing child death and reducing hospital admissions caused by unintentional and deliberate injuries to children.
3. CDOP Scope and Analysis
The CDOP will collect and analyse information surrounding the death of any child who is a resident of Cambridgeshire and Peterborough. To gather this information an electronic system called eCDOP is used, which has several forms that professionals may be required to complete:
- Form A – a notification form which professionals use to notify the CDOP manager that a child/young person has died.
- Form B – an agency reporting form used to gather specific and detailed information from agencies involved a child/young person’s life and care prior to and during death.
- Form C – a panel analysis form completed by the CDOP members during case discussion, looking at contributory factors, modifiable factors and recommendations/learning.
All information gathered within the eCDOP system is fed into the National Child Mortality Database (NCMD) who monitor CDOP’s nationally, looking at themes surrounding child deaths and recommendations.
The CDOP members meet on a quarterly basis to review cases and consider the factors within the Form C. During the meeting the CDOP members have the following information available to them to support their assessment:
- Case information from Health, Police, Local Authority/Children’s Social Care, Education, and any other relevant agencies involved in the child’s life via the Form B.
- Post-mortem reports, Coroner’s enquiries, and inquest bundles.
- Minutes from the JAR meeting(s).
- CSPR reports, including Individual Management Reports (IMR’s)
4. Consent and confidentiality
The receiving and processing of information about a child who has died for Child Death Review purposes is statutory and therefore cannot be refused by a parent or guardian. Therefore, it is disingenuous to seek consent as it cannot be refused. However, it is best practice to inform those with parental consent of the process and explain its purpose. This should be carried out by the named support worker during the initial investigation and support phase.
Whilst a deceased person is no longer subject to the General Data Protection Regulations and does not have a legal right to withhold their personal information, care must be taken with all personal and sensitive information as though the person held such rights. Information should only be shared with those who need to know, as governed by the Caldicott Principles, the General Data Protection Regulations and Working Together to Safeguard Children.
All member agencies must be aware of the need to share information about all child deaths with the panel in order that CDOP can fulfill its statutory duty.
All members of the panel must respect and maintain confidentiality of the children who are being reviewed.
All member agencies agree that the CDOP is the data controller for each individual case summary, but not individual agency records. A summary is a collated from information that agencies that have inputted into eCDOP.
Information brought to the panel will be anonymised. However, some cases may have elements of identifiable information that must be shared to properly understand the death.
Members of the panel, or observers, are required when they join the panel, to sign a confidentiality agreement that includes requirements about sharing and securely storing information (see appendix three).
CDOP members must not disclose information from discussions which take place within the meeting, other than as part of the agency responsibilities of that individual. Public statements regarding the general purpose of the child death review process may be made if they do not identify a specific case.
Anonymous reports and timelines created for the use of CDOP will be deleted on closure of a case and only stored within eCDOP.
5. Membership of the CDOP meetings
The CDOP members meet on a quarterly basis to review cases once all information has been gathered, the CDOP membership consists of representatives from:
- Cambridgeshire and Peterborough Integrated Care Board
- Cambridgeshire Constabulary
- Cambridgeshire and Peterborough Safeguarding Partnership Board
- North West Anglia NHS Foundation Trust
- Cambridgeshire University Hospitals NHS Foundation Trust
- Cambridgeshire Community Services NHS Trust
- Cambridgeshire and Peterborough NHS Foundation Trust
- East Anglian Children’s Hospice
- Public Health England
- Cambridgeshire County Council Children’s Social Care
- Peterborough City Council Children’s Social Care
- Education
- East of England Ambulance Service NHS Trust
- Primary Care
The CDOP chair can co-opt other professionals to the membership where appropriate, such as the Road Safety Partnership or LeDeR representative if they better reflect the characteristics of the local population, provide expertise for certain types of death, or provide perspective from an independent sector.
The CDOP chair and vice chair are accountable to the Child Death Review partners.
The CDOP meeting will be quorate if there are representatives from each of the local Health and Social Care organisations.
6. Children who die in this area but are not usually residents
In some instances, children that die in Cambridgeshire and Peterborough do not usually reside here, in this instance the CDOP will:
- Inform the CDOP coordinator/manager in the child’s Local Authority area.
- Agree between areas how to support the gathering and reviewing of information.
- For unexpected deaths, the local rapid response team will consider a joint visit with Police to the scene of the death.
- Request a copy of the completed form C to take forward any local learning, for example, learning about road traffic collision spots.
7. Death of a local child outside of area
When a child resident of Cambridgeshire and Peterborough dies out of area the Cambridgeshire & Peterborough CDOP manager will liaise with their counterpart and agree their respective roles. The death will be counted within local numbers, and unless there is a reason to do otherwise the child’s death will be discussed at their local CDOP as per the child’s usual place of residence. The Coroner will be identified by the place of death, not the child’s home address.
If a child dies outside of the jurisdiction of the UK, the CDOP manager will seek information about the death and a review will take place as usual. The Coroner for the Foreign and Commonwealth Office may be able to assist in gathering information on behalf of the CDOP.
Children who die in hospital, outside of area, may be subject to a local child death review meeting held by hospital staff, information and learning from this should be shared with the Cambridgeshire and Peterborough CDOP.
Children, where parental responsibility is shared with the Local Authority, (e.g., children in care) may be placed in another county, however their death would be reviewed by CDOP in their normal area of residence in conjunction with social care providers and local children’s services.
The Coroners Investigations Regulations 2013[3] places a duty on Coroners to inform the Child Death Review partners for the area in which the child died, or the child’s body was found, where the Coroner decides to investigate or directs that a post-mortem should take place. The Coroner must provide to the child death review partners all information held by the Coroner relating to the child’s death.
Where the Coroner makes a report to prevent further deaths, a copy must be sent to the Child Death Review Partners. On receipt of an initial report of a death of a child, the Child Death Review Partners should inform the Coroner of the address(es) (including email address(es)) to which future information should be supplied. If any information comes to the attention of the child death review partners which it believes should be drawn to the attention of the relevant Coroner, then the child death review partners should supply it to the Coroner as a matter of urgency.
8. Professional and family support
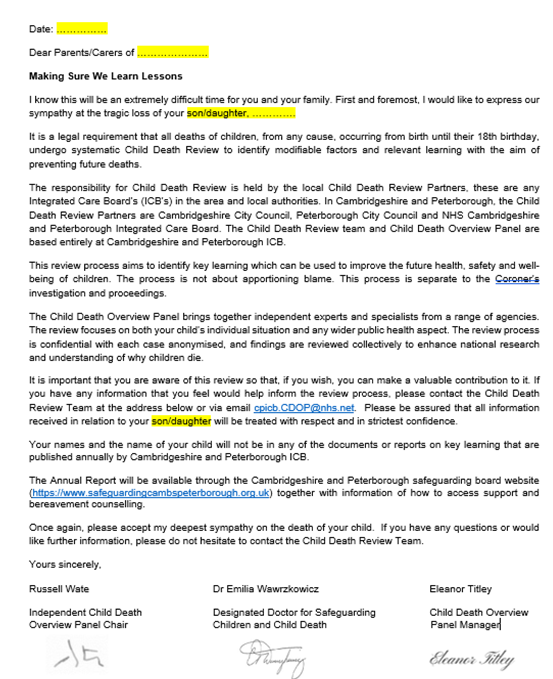
The CDOP will write to parents/families/cares following notification of a child death, offering condolences, explaining the CDOP process, providing bereavement support sign posting and the opportunity for them to share any thoughts into the CDOP (see appendix two).
If a JAR is held following an unexpected child death the group will agree on how best to support parents/families/carers following a child death, with a lead professional being identified to offer this to the deceased’s family.
In the event of a death by suicide the CDOP manager will liaise with relevant educational settings, i.e., schools and colleges, to ensure information is shared in a timely manner, as well as offering and organizing bereavement support via the Samaritans charity for teachers and pupils. The Samaritans will support schools in sharing information with other pupils, holding assemblies with affected year groups and supporting friendship groups, teachers and parents. Multi-agency guidance has been created for supporting schools and colleges in responding to suicide in teenagers.
All professionals involved in the CDOP process can request a further JAR meeting once post-mortem findings have been completed. Professionals are also able to discuss cases they are involved in with the Designated Doctor for Child Death should they require further support.
Post-mortem findings are shared with key health professionals, usually the child’s GP and Doctor from the acute health setting. These professionals are expected to share the post-mortem findings with families/carers, rather than this being shared via the Coroner’s office.
9. Learning from child deaths
The CDOP will monitor and advise Cambridgeshire and Peterborough Safeguarding Partnership Board on the resources and training required locally to ensure an effective inter-agency response to child deaths.
The CDOP may identify public health or welfare issues and report these to the Director of Public Health to consider how best to address these and the implications for both the commissioning of services and training.
The CDOP process will contribute to regional and national initiatives to identify lessons on the prevention of child deaths, to monitor advice and research nationally/internationally with knowledge about effective interventions.
Using advice and recommendations from the CDOP the Cambridgeshire and Peterborough Safeguarding Partnership Board will:
- Disseminate the findings and lessons to all relevant organisations.
- Ensure that relevant findings inform single agency plans.
- Act on any recommendations to improve policy, professional practice, and interagency working to safeguard and promote the welfare of children.
- Ensure that data relating to child deaths is submitted to relevant local, regional, and national initiatives including the Joint Strategic Needs Assessment to identify lessons on the prevention of avoidable factors in child deaths, hospital admissions, accidents, and morbidity.
Some child deaths may be best reviewed at a themed meeting. A themed meeting is one where CDR partners arrange for a single CDOP, or neighbouring CDOPs, to collectively review child deaths from a particular cause or group of causes. Such arrangements allow appropriate professional experts to be present at the panel to inform discussions, and/or allow easier identification of themes when the number of deaths from a particular cause is small.
Appendix 1
Appendix 2
CDOP Letter to Parents/Carer’s
Appendix 3
CDOP Confidentiality Statement
The purpose of the Child Death Overview Panel is to conduct a thorough review of all deaths of those under 18 years old in Cambridgeshire and Peterborough to better understand how and why children die and to take action to prevent further deaths.
To assure a coordinated response that fully addresses all systematic concerns surrounding child deaths, all relevant data should be shared and reviewed by the CDOP team, as permitted within the stipulations of the Data Protection Act, including historical information concerning the deceased child, their family, and the circumstances surrounding their death. Much of this information is protected from public disclosure.
The Cambridgeshire and Peterborough protocol for the Child Death Overview Panel and the Cambridgeshire and Peterborough Safeguarding Partnership Boards protocol for child death reviews stipulate that; ‘in no case will any team member disclose any information regarding team discussion outside the meeting other than pursuant to the mandated agency responsibilities of that individual. Public statements about the general purpose of the child death review process may be made, as long as they are not identified with any specific case.’
The undersigned agrees to abide by the terms of this confidentiality policy:
Name: | Signature: |
|
|
Date: |
Agency: |
|
|