Issue No: | 1 |
Document Owner: | Cambridgeshire Safeguarding Children Partnership & Peterborough Safeguarding Children Partnership |
Date Approved: | 9 December 2025 |
Review Date: | December 2026 |
Table of Contents
To view the guidance as a pdf, please click on this link Guidance for CSPRs (Updated 2025)
Introduction
This document sets out the arrangements and local processes by which both the Cambridgeshire and Peterborough Safeguarding Children Partnerships will determine when to trigger and undertake a Rapid Review where a serious safeguarding case is identified, including the actions for cases that do not meet the criteria. The processes are informed by the National Child Safeguarding Practice Review Panel’s Guidance for Safeguarding Partners, published June 2025.
The Children and Social Work Act 2017, and Statutory Guidance Working Together to Safeguard Children, provides the legal framework for multi-agency safeguarding arrangements and the requirement for local areas to undertake a Rapid Review where a serious safeguarding case is identified, and such a review is considered appropriate to identify improvements to practice.
This guidance provides professionals in Cambridgeshire and Peterborough with a step-by-step guide to follow when undertaking or participating in a Local Child Safeguarding Practice Review. It describes the approach, order of events and related timescales whilst also highlighting the key statutory elements outlined in Working Together to Safeguard Children 2023. It also outlines responsibilities for key people at every stage of the process and includes template documents and letters.
Strategic Leadership and Governance
The statutory partners are responsible for ensuring that when cases meet the criteria for Rapid Reviews and Child Safeguarding Practice Reviews (CSPRs), they have robust processes that meet the standards expected by the National Child Safeguarding Practice Review Panel (hereafter referred to as the National Panel).
The Delegated Safeguarding partners take decisions on behalf of their organisations / agency and have power to commit resourcing, change policy, and hold their organisation to account in order to effect and implement local changes. They make the final decisions on commissioning local CSPRs.
Governance for these arrangements sit with the Safeguarding Partnerships CSPR Subgroup, which is made up of senior representatives from Children Services, Police, ICB with additional members from Education, and Health trusts.
The chair of the subgroup is responsible for guiding the functions of the panel and ensuring that decision making is exercised equally by the partners’ delegated representatives, taking the lead on any issues that arise between the partners. The chair is also responsible for ensuring that learning and key messages are reported to the Safeguarding Partnerships and the partners are alert to thematic issues as well as examples of good practice.
Information Sharing
Information sharing is essential to safeguard and promote the welfare of children and young people. Effective Child Safeguarding Practice Reviews are equally dependent on all relevant partners sharing the information they hold about the case and associated professional practice.
The Safeguarding Partners have the formal authority to request information to support both national and local Child Safeguarding Practice Reviews and the power to take legal action if information is withheld without good reason.
All agencies will be expected to share relevant information within the timescales requested. This may, when necessary, include sharing information without consent (such as where there is an ongoing police investigation). This includes information about parents, guardians and other family members as well as the child(ren) who are subject of the review.
Where a request is for health records this applies to all records of NHS commissioned care whether provided under the NHS or in the independent or voluntary sector.
When making requests for information, the Safeguarding Partners will consider their responsibilities under the relevant information law and have regard to guidance provided by the Information Commissioner’s Office.
Good practice principles around information sharing will always be followed, particularly around ‘how’ information is shared. For example, when responding to requests for information, agencies should:
- Identify how much information to share; distinguish fact from opinion;
- Ensure that they give the right information to the right individual;
- Ensure that they share information securely;
- Where possible, be transparent with the individual, informing them that that the information has been shared (as long as doing so does not create or increase the risk of harm);
- Record all information sharing decisions and reasons in line with organisational procedures.
In the case of any disagreement or failure to comply with a formal information request, the Independent Lead Reviewer or member of an Independent Review Team will refer the issue to the Case Review Subgroup who will seek to resolve this with the strategic Safeguarding Lead for the agency concerned. If a prompt resolution cannot be found, the issue will be escalated to the Delegated Safeguarding Partner for formal resolution.
Decision Making around reviews
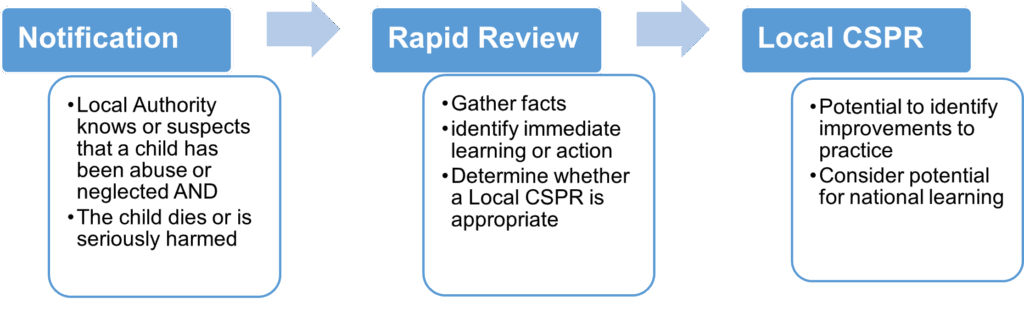
As outlined in Working Together to Safeguard Children 2023, and the National Panel’s Guidance; There are three key stages in the process of learning from serious incidents:
- Serious incident notification to National Panel shared with Ofsted and the DfE.
- Rapid review which should be completed within 15 working days of notification.
- Consideration of an LCSPR or national review.
Serious Child Safeguarding Incidents
What is a Serious Child Safeguarding Incident?
Working Together 2023 states that the safeguarding partners must identify, commission and oversee the review of serious child safeguarding cases.
Serious child Safeguarding cases are those in which:
- Abuse or neglect of a child in known or suspected
- The child has died or been seriously harmed.
Is it serious harm?
Working Together 2023 describes serious harm as including (but not limited to) serious and/or long-term impairment of a child’s mental health or intellectual, emotional, social, or behavioural development as a result of neglect or abuse. It also states that when making decisions, judgement should be exercised where impairment is likely to be long-term, even if this is not immediately certain. Even if a child recovers, including from a one-off incident, serious harm may have still occurred.
The threshold for notification to the National Panel is distinct from the threshold for children suffering “significant harm” that may lead to, for example, time on a child protection plan or children becoming subject to public care proceedings. Whilst it is likely that many children who have suffered “significant harm” will live with the long-term physical and emotional consequences of that, “serious harm” is a higher-level threshold for the exceptional incidents.
The judgement about whether the level of harm to a child is serious is often quite straight forward. This may be because the child has a life-changing physical injury, or an injury that is clearly life-threatening – for example, requiring resuscitation or intensive care treatment. It might also be because what has happened to a child is quite exceptional and the harm suffered will have severe long-term consequences for their health and well-being. However, the judgement about some incidents may be less straightforward. It is important that safeguarding partners use their professional judgement to determine whether the harm to a child should be deemed serious.
Notifications of Serious Incidents
16C (1) of the Children Act 2004 (as amended by the Children and Social Work Act 2017) states: Where a local authority in England knows or suspects that a child has been abused or neglected, the local authority must notify the Child Safeguarding Practice Review Panel if – a) the child dies or is seriously harmed in the local authorities area, or b) while normally resident in the local authority’s area, the child dies or is seriously harmed outside England. |
The local authority should notify any incident that meets the above criteria to the National Panel via the Child Safeguarding Online Notification System, within five working days of becoming aware it has happened. A copy of the notification will automatically be sent to the DfE and Ofsted.
Although the responsibility to notify rests on the local authority, it is for the statutory safeguarding partners to agree which incidents should be notified in their local area. (Working Together 2023 – Chapter 5, para. 330).
Deaths of a Looked-after children and Care Leavers
All deaths of looked after children, including deaths by suicide, accidents and medical causes, must be notified to the DfE and Ofsted via the Child Safeguarding Online Notification System. However, unless abuse or neglect was known or suspected to have contributed directly to the death, these cases do not need a rapid review. (Working Together 2023 – Chapter 5, para 331 and National Panel Guidance for Safeguarding Partners – Chapter 2, para 2.13 – 2.14))
Death of Care-leavers
The local authority should notify the DfE and Ofsted of the death of a care leaver up to and including the age of 24 via the Child Safeguarding Online Notification System. The death of a care leaver does not require a rapid review, however, safeguarding partners must consider whether the criteria for a serious incident have been met. (Working Together 2023 – Chapter 5, para 332)
Non-recent abuse
If safeguarding partners identify young people over the age of 18 who have experienced serious harm and neglect or abuse when they were a child, and information sharing suggests that there are learning opportunities for the local system. When the primary harm for an over 18-year-old is related to the abuse and neglect they experienced as a child, safeguarding partners should consider whether to follow Safeguarding Adults Review or Child Safeguarding Practice Review process as most appropriate. Partners should take into consideration the time that has elapsed since the harm occurred, the opportunities for learning and whether the learning principally relates to adult or children services. As the purpose of completing reviews is to generate learning, it is up to statutory partners to decide if the learning is sufficiently relevant to justify the investment of resource these reviews would entail. If partners decide to use the Child Safeguarding process, a notification should be submitted with an approximate date of when the incident occurred to evidence that the harm occurred during childhood, followed by a rapid review. (National Panel Guidance for Safeguarding Partners – Chapter 2, para 2.8 – 2.12)
Referring a case for consideration
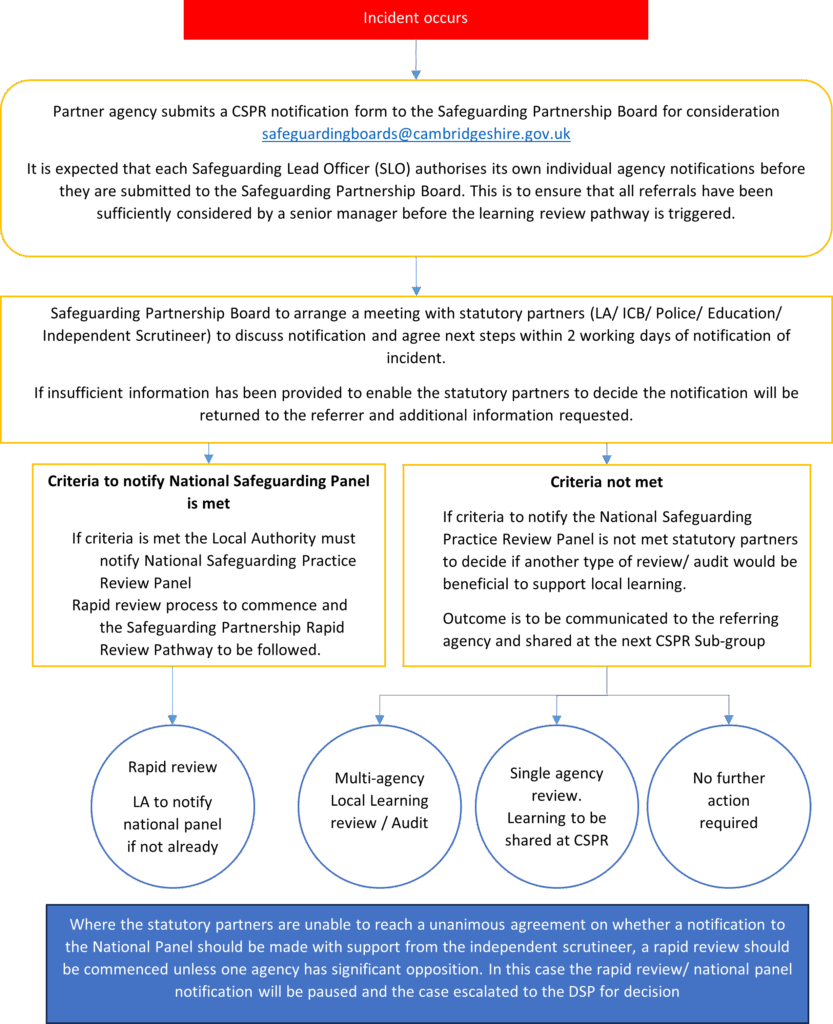
Where an agency becomes aware of an incident that meets the above criteria, that agency must complete a notification form (Appendix 1) immediately and send to their Safeguarding Lead Officer (SLO) for authorisation. Once authorised by the SLO, the notification form should be submitted to the Safeguarding Children’s Partnership via safeguardingboards@cambridgeshire.gov.uk, who will arrange a meeting with the statutory partners and independent scrutineer to be held within two days to determine whether a Serious Incident Notification should be made and agree the next steps.
In order to reach a decision, the statutory partners will:
- Review the referral
- Identify if their own agency holds further information to inform the decision making
- Consider whether or not the criteria for a Serious Incident Notification has been met and so warrants a notification to the National Child Safeguarding Practice Review Panel
- Consider whether a rapid review is required
Outcomes of case consideration
- Notification made and progress to Rapid Review
- No Notification made and No Further Action
In some cases, it may be appropriate to take no further action with a case referral. - No notification made and progress to a Single Agency Review
Where the issue relates to a single agency, then that agency may be tasked to take forward an appropriate review and report back its findings to the CSPR subgroup. - No Notification made and progress to a Multi-Agency Review
If the threshold for a notification has not been met, but there is potential for multi-agency learning, a non-statutory review may be undertaken where learning is limited or less complex.
Notification of Significant Child Safeguarding Incident Pathway
Rapid Reviews
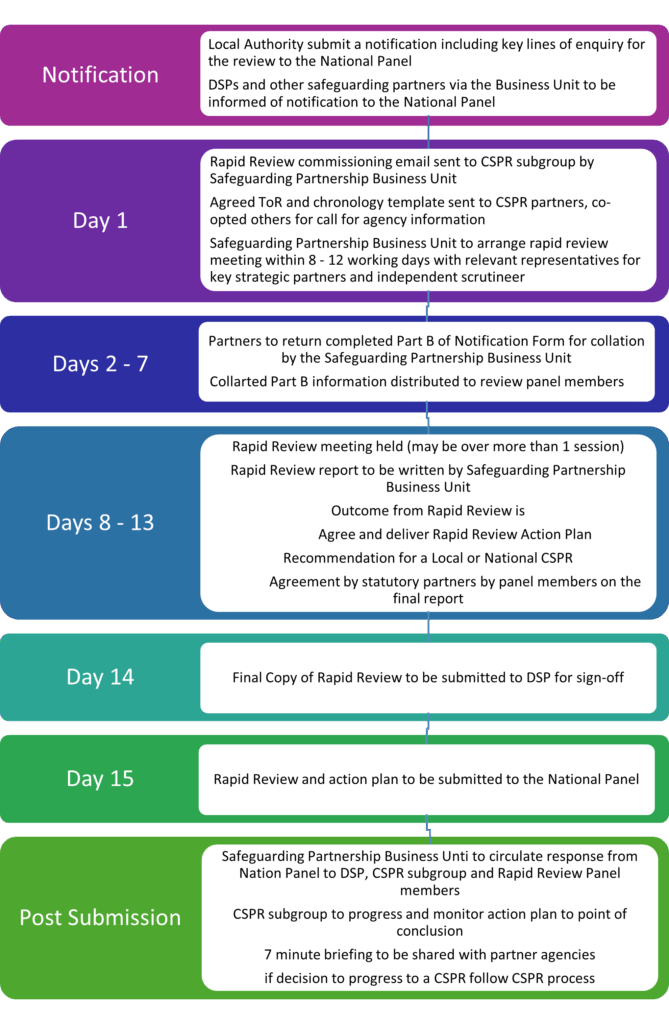
Following the safeguarding partners’ decision to notify the National Panel about a serious incident, the safeguarding partners must complete a rapid review of the child’s experience within 15 working days from the date the notification was sent as outlined in the National Panel’s guidance.
A flow chart setting out the key stages and suggested timescales to meet the prescribed submission target is included at the end of this section.
The purpose of the rapid review is to:
- Gather the facts about the case, as far as they can be readily established, including details of agency involvement and an analysis of key practice episodes.
- Discuss whether any immediate action is needed to ensure children’s safeguarding and share any learning appropriately
- Consider the potential for identifying improvements to safeguard and promote the welfare of children
- Understand the context of children’s and families’ lives including how racism and other inequalities related to other protected characteristics “including disability” may have influenced children’s and families’ experiences and the quality of practice.
- Decide what steps they should take next, including whether to undertake an Local Child Safeguarding Practice Review.
Cross Border
Where a case involves services delivered across more than one safeguarding partnership, partners should liaise and agree which safeguarding partnership will lead the rapid review. Normally this would be the safeguarding partnership in the area where the child usually resides.
Where a child is/was placed out of area, the originating authority which placed the child retains legal responsibility for the child and will take the lead on the review with input from the receiving authority.
Initial Scoping, Information Sharing and the Securing of Records
All relevant agencies who currently have, or had recent, involvement with the child or family will be required to contribute to the Rapid Review. The purpose of the initial scoping is to gather the facts about the case, including determining the extent of agency involvement with the child and their family. More detailed information may be sought if the Rapid Review concludes the case has the potential to identify further learning and a decision is made to recommend a national or local Child Safeguarding Practice Review.
The Safeguarding Partnerships’ Business Unit will send out an Initial Scoping template (Appendix 2) to identified agency colleagues with a request for completion of the form and to be returned to the Business Unit within 5 working days.
The time period to be considered would be determined based on the circumstances of the case up to a maximum 24-month period. Agencies will only be expected to provide information over 24-months if it is deemed relevant.
The completed templates must be quality assured by the individual agencies prior to being submitted. The individual templates will be collated in to a single composite document to be circulated ahead of the Rapid Review meeting.
Where possible, agencies should also secure all records/files in relation to the case, ensuring they are removed to a secure place, where they are not accessible to agency personnel other than through a nominated representative. Where access to the records is required for ongoing case work, a copy should be made and secured.
The lead agency working with the child/family may be asked to prepare a full and accurate genogram to assist the clarification of family relationships and dynamics. This will be shared with other agencies at Panel meetings and will be updated based on any additional information on the family provided by these agencies.
Setting the date for the Rapid Review Meeting
The date of the Rapid Review meeting should be set as soon as possible before the Initial Scoping has been sent out. The Rapid Review meeting should be scheduled between 8 and 12 working days of receiving the referral. This will allow for analysis of the Initial Scoping to establish the key events in the child’s life and inform the Rapid Review whilst also allowing sufficient time to prepare the necessary documents for the National Panel.
Wherever possible the Referral, collated Initial Scoping and Genogram will be shared with participants in advance of the meeting. However, it is recognised that it may on occasion be necessary to share documentation at the meeting.
Rapid Review Meeting
The Rapid Review meeting will include representatives from each of the Safeguarding Partners (Local Authority Children’s Services, Police, ICB) and any other agencies who had significant involvement with the family as well as the Independent Scrutineer. Education services should be represented when children are of statutory school age. Childcare settings should be represented if children are attending this provision.
The Rapid Review meeting will:
- Review the facts about the case as they are known;
- Discuss whether any immediate action is needed to ensure children’s safety;
- Identify immediate learning that can be acted upon and agree how this will be shared.
- Consider if the case raises any issues that are complex or of national importance such that a national review may be appropriate, and if so, inform the panel.
- Consider the child’s true lived experience and how can their voice be heard in the review.
- Consider how race, culture, faith, and ethnicity of the child and/or family was considered by practitioners and did cultural considerations impact on practice.
- Consider how any disability, physical or mental health issues, and any identity issues in the child and/or family impact on the child’s lived experience and on practice
- Consider whether there were any risk factors present or absent and the impact
- Highlight good practice
- Decide whether or not to undertake a local Child Safeguarding Practice Review and record a clear rationale behind the decision. Where it is agreed to proceed with a local CSPR, the meeting should agree the Key Lines of Enquiry (KLoE)
- Record actions to take forward with appropriate agencies.
Deciding whether to conduct an Local CSPR
Following discussion about the case, each of the three statutory partners (Police, ICB and relevant LA) will get a single vote, to decide whether or not to undertake a Child Safeguarding Practice Review. Where there is disagreement, this should be recorded and shared with the Delegated Safeguarding Partners.
A thorough Rapid Review may mean that there is no need for a separate Local Child Safeguarding Practice Review and areas can move quickly to implement learning across the system.
Safeguarding partners need to be clear what the benefit would be of conducting an Local CSPR for example, is there new learning that has not yet been identified already through local safeguarding systems. The National Panel makes it clear that following a rapid review “any further review of a case should be referred to as an LCSPR”
Rapid Review Report
Following the Rapid Review meeting, the author will write up the Rapid Review report which should include:
- Date of Birth, sex, ethnicity of family members, whether the child has any known disability
- Immediate safeguarding arrangements for any of the children involved
- The child’s voice including a summary of their identity and characteristics and how these impacted upon their experiences
- How children’s vulnerabilities and risk of harm were recognised and responded to
- Family structure and relevant history and background information, including details of all the children in the family, genogram, information about the parents and any significant adults, including ages and any known physical or mental health problems or disabilities.
- Information about the alleged perpetrator of the harm, including involvement with relevant agencies
- A concise summary of the facts about the serious harm and relevant context.
- The agencies involved in the rapid review, explaining any gaps in agency involvement
Rapid review reports should identify learning and recommendations, include:
- Information about the learning that has already been capture, and good practice and how this is being shared across the system.
- If any published national or local reviews or relevant research can be referenced and used to support local learning.
- If there are issues of national significance for the Panel to consider, including the rationale for any recommendations.
- Recommendations for creating the right conditions for good practice to flourish which are the responsibility of strategic leaders alongside managers and practitioners
- An action plan with clear agency and partnership actions to take forward including timescales.
- A clear decision and rationale as to whether the criteria for an LCSPR have been met and on what grounds, and if not, why not.
- Key lines of enquiry for any LCSPR.
On completion of the Rapid Review, the three representatives for the statutory partners should agree the Rapid Review Report. Once agreed, the Report will be shared with the Delegated Safeguarding Partners for sign off and provide their observations of the review together with their decision and rationale for any decision.
Sharing the Outcome of the Rapid Review
On day 15 of the Rapid Review process, the rapid review and outcome along with a concise action plan with clear timescales will be sent to the National Panel, DfE and Ofsted (Mailbox.NationalReviewPanel@education.gov.uk)
Individual agencies should notify their own inspectorate bodies as required.
All information shared as part of the rapid review process should be treated as confidential
Rapid Reviews Flowchart
Local Child Safeguarding Practice Reviews
Purpose of Child Safeguarding Practice Reviews
The purpose of child safeguarding practice reviews is to identify improvements to be made to safeguard and promote the welfare of children. Understanding whether there are systemic issues, and whether and how policy and practice need to change, is critical to the system being dynamic and self-improving. Reviews should also seek to identify areas of good practice.
Reviews should seek to prevent or reduce the risk of recurrence of similar incidents. They are not conducted to hold individuals, organisations or agencies to account, as there are other processes for that purpose, including through employment law and disciplinary procedures, professional regulation and, in exceptional cases, criminal proceedings. These processes may be carried out alongside reviews or at a later stage. Employers should consider whether any disciplinary action should be taken against practitioners whose conduct and/or practice falls below acceptable standards and should refer to their regulatory body as appropriate.
Criteria for a local safeguarding practice review
Safeguarding Partners are required to consider the criteria and guidance when determining whether to carry out a Local Child Safeguarding Practice Review. They must take into account whether the case highlights[1]:
- improvements needed to safeguard and promote the welfare of children, including where those improvements have been previously identified;
- recurrent themes in the safeguarding and promotion of the welfare of children which may require legislation or changes to guidance;
- concerns regarding two or more organisations or agencies working together effectively to safeguard and promote the welfare of children;
They should also have regard to the following circumstances where:
- the National Panel has considered the rapid review and has concluded a local review may be more appropriate;
- they have cause for concern about the actions of a single agency or lack of agency involvement;
- more than one local authority, police area or ICB is involved, including the examples where a family has moved around and there is evidence that this increases the family’s vulnerability;
- the experience may raise issues related to safeguarding or promoting the welfare of children in institutional settings, including secure children’s homes, young offenders’ institutions and secure training centres, and all settings where children may be detained under the Mental Health Act 1983 or Mental Capacity Act 2005.
Approach and Principles
Each Child Safeguarding Practice Review will be proportionate to the circumstances of the case and focus on the potential learning. Each review will be undertaken using the most appropriate methodology to identify and maximise learning to improve both frontline safeguarding practice and organisational structures.
Where there are multiple incidents occurring with similar themes, the safeguarding partners may decide to undertake thematic CSPRs. When these are undertaken, the voice, experiences and individual characteristics of each child and family are to be reflected within the review
Specifically all reviews will be conducted in a way which:
- reflects the child’s perspective and family context;
- considers and analyses frontline practice as well as organisational structures and learning;
- establishes the reasons why events occurred as they did;
- identifies clear learning that will improve outcomes for children
Practitioners will be fully involved in reviews and invited to contribute their perspectives without fear of being blamed for actions they took in good faith.
CSPR Panel
Once the decision has been made that a local Child Safeguarding Practice Review will be undertaken, a Panel will be established a time limited activity operating as a group to support the completion of the Child Safeguarding Practice Review.
The statutory safeguarding partners and all involved agencies will be required to identify relevant representatives for the CSPR panel, which may be the same colleague who sat on the Rapid Review meeting. Subject matter experts may also be invited to become members of the panel.
Panel meetings will be organised throughout the process, as required.
The role of panel members are to:
- ensure the terms of reference for the CSPR clearly identifies the key lines of enquiry for the review, based on the learning from the Rapid Review, and National Panel’s feedback
- work in collaboration with the Business Unit to identify a reviewer who is independent of the case
- Identify gaps in panel membership and agency information
- Ensure the review is progressed at pace to identify learning as quickly as possible, and within the timescales expected in Working Together to Safeguard Children
- Ensure all required, requested and appropriate information is provided to the reviewer
- support the reviewer to contact family members (as appropriate)
- identify appropriate practitioners to be involved in any information gathering event / workshop
- be a conduit back to their organisation for any specific requests from the reviewer or review process.
- provide feedback to the reviewer when a draft report is produced, to ensure accuracy of the content.
- Agree the recommendations arising from the review
In addition to the above, Panel members will be required to
- Actively participate in the panel’s discussions sharing all relevant information. This enables the panel as a whole and the reviewer to develop a comprehensive set of information to identify learning
- Ensure that agency recommendations are specific, measurable, achievable, relevant and time-bound (SMART)
- Act as a ‘critical friend’ to other panel members and help encourage reflection of the issues being discussed.
- Value the learning from different inputs and stay open to new ways of doing things.
- Be present in the meeting, and don’t attend to non-meeting business. Listen attentively to others and don’t interrupt or have side conversations.
- Communicate with their chief officer/s and / or senior management team on progress of the review, in order to cultivate ownership of the conclusions, and avoid any surprises about the learning being identified
- Supporting members of staff from their organisation attending review events (i.e. information gathering events). This includes providing suitable support and briefing before, during and after the event.
- Provide feedback to staff at all levels within their organisation on the progress and findings from the review
Panel members will support the reviewer to scrutinise the information provided by agencies. Panel members will also provide local context and challenge to the analysis of professional practice and the identification of learning. Where an agency report is not of the quality expected, the reviewer will make contact with the relevant agency via the panel representative and ask for the report to be revised and resubmitted in a timely manner.
The police representative on the panel will be responsible for liaising with the Senior Investigating Officer, Crown Prosecution Service, and for co-ordination of family liaison.
Appointing the Reviewer
An independent reviewer will usually be appointed to manage the review process, chair meetings of the panel, facilitate workshops and author the final report.
Where reviewers are internal to the safeguarding partnership, assurance should be sought that they meet the following requirements set out in Working Together to Safeguard Children.
The reviewer should have:
|
The Safeguarding Partners will inform the National Panel, Ofsted and the Department for Education of the name of any reviewer commissioned via email to:
Mailbox.NationalReviewPanel@education.gov.uk
Timescale for Completion of the Review
Reviews will vary in their breadth and complexity but in all cases learning should be identified and acted upon as quickly as possible. This includes learning identified before the review has formally commenced and while it is in progress.
All statutory local Child Safeguarding Practice Reviews are expected to be completed within six months from the date of the decision to initiate a review.
Sometimes the complexity of a case does not become apparent until the review is in progress. For example, the police undertaking a criminal investigation may request a delay to the review due to involving specific key individuals. Any delays need to be considered by the relevant Case Review Subgroup as soon as they arise. If the delay will prevent the publication of the final report within six months, the National Panel and Secretary of State should be informed and provided with the reason for the delay.
The interface with other statutory processes and parallel investigations including criminal proceedings
There may be a criminal investigation, a coroner’s investigation and / or professional body disciplinary procedures, and/or another type of formal review[2] running alongside a local or national CSPR. It is anticipated that a local Child Safeguarding Practice Review will go ahead unless there are clear reasons not to.
The CSPR panel and safeguarding partners will agree how they will work alongside other processes to reduce potential duplication for families and staff.
Where a Coroners Court requests sight of a case review report or information relating to the review this will be shared in line with Worcestershire County Council and Worcestershire Safeguarding Children Board v HM Coroner for the County of Worcestershire [2013]
Agencies should be aware that a request may be made by the Police or Court for chronologies/ reports to be disclosed when information is being gathered for a criminal case. If requested, the Safeguarding Children’s Partnership will not provide a copy of these documents but will forward contact details of safeguarding partners to the Officer seeking disclosure so that direct contact can be made.
The Crown Prosecution Service has issued guidance about how any risks to criminal proceedings can best be managed and mitigated. Protocol for Liaison and Information Exchange when criminal proceedings coincide with Child Safeguarding Practice Reviews in England | The Crown Prosecution Service
Legal Advice
Consideration will be given to whether legal advice should be sought at the outset, during the review or prior to publication.
Engaging Children and Family Members
Family members, siblings and surviving children, will be informed of the review, and invited to contribute unless there is a strong reason not to do so. The initial panel meeting will discuss family involvement and agree an approach that will sensitively manage their expectations and ensure they understand the process.
Personal contact should be made whenever possible by the most appropriate professional and the family provided with a letter and / or leaflet to explain and introduce the review process and reviewer.
Family engagement will normally be led by the reviewer and conversations should take place early in the process, preferably prior to information gathering events. However, engagement may not be possible until the outcome of any criminal proceedings. This will be judged on a case-by-case basis and involve liaison with the Senior Investigating Officer.
Family members may decide not to take part in the review. All reasons for non-involvement of family members (for example, parallel proceedings or the choice of the individual) will be documented in the final report.
Agreeing Terms of Reference and Key Lines of Enquiry
The Case Review Panel and reviewer will develop and formally agree the terms of reference at an early stage which will set out the scope and key lines of enquiry for the review.
The time period / scope covered by the review should reflect the potential learning likely to be achieved. Where possible, it should be short and as recent as possible whilst balancing against the need to understand the patter of child abuse or neglect and whether early interventions could have been beneficial.
The Key Lines of Enquiry (KLoE) identified during the Rapid Review will be considered and agreed however these may be revised during the review if more information becomes available.
Methodology
Working Together to Safeguard Children does not specify the methodology that should be used in Reviews, but there is an explicit expectation that ‘principles of the systems methodology recommended by the Munro Report’ will be ‘taken into account’ by the Safeguarding Partners when agreeing the method by which the review will be conducted
Each case will be examined individually, and the methodology will be adapted to meet the specific needs of the case, to ensure a proportionate response, and to maximise learning to improve both frontline safeguarding practice and organisational structures.
Agency Action and Expectations
All agencies which provided services to the family during the time period specified in the Terms of Reference will be formally requested to participate in the review process. The extent of agency engagement will be dependent on the type of review commissioned, the specific Terms of Reference and methodology chosen.
Each organisation should have an identified Safeguarding Lead to act as a single point of contact for the co-ordination and support of the review process.
Agencies should ensure that all requests for information are acted upon in a timely fashion, and practitioners are released to participate in the review. Agencies should also provide support to their staff who are affected by the case where required.
Information Collection and Collation
The terms of reference will specify the methods of information collection that will be used in the review. This may include chronologies (of key events and/or organisational changes), Agency Reports, source materials, or a combination of these.
Chronologies
Where chronologies are used, all relevant agencies will be asked to complete a chronology of their agency’s involvement. They may also be asked to produce a chronology of any organisational changes which may have impacted on frontline practice during the review period.
Individual agency chronologies are likely to be collated to produce an Integrated Key Events Chronology, which may be colour coded to facilitate an ‘at a glance’ overview of agency involvement.
Chronologies will be used as a tool to support analysis of events and to identify key Practice Learning Events.
Agency Reports
Agency reports can be used to analyse an agency’s involvement with the child and family and any themes that have emerged. These should outline any potential learning for the agency or for multi-agency arrangements and should include information about actions already undertaken.
Reviews may wish to draw on wider evidence related to the case. For example, the context of the local area, data and analysis related to agencies and services, national and international evidence, and learning from other local CSPRs and / or national reviews.
Information Gathering Events / Reflective Learning Workshops
Information Gathering Events / Reflective Learning Workshops provide a forum for frontline professionals and their line managers to come together in a respectful, positive and supportive environment to consider the circumstances surrounding the case and the reasons why actions were taken. This enables the reviewer to identify important multi-agency learning.
Panel members will ensure a list of appropriate professionals that should be invited to attend the workshop is sent to the Business Unit to allow participants are given plenty of notice. Invites will be accompanied by a short briefing document which explains the purpose of the event and the importance of attending.
Panel members should inform the frontline professionals and their line managers of the workshop and ensure staff receives support before, during and after the event.
To maximise the learning, all agencies involved in the review will be expected to ensure that appropriate staff attend the workshop, however, it is preferable that only those who have had some form of direct involvement with the child and family attends.
Capturing Improvements and Taking Corrective Action while the Review is in Progress
The Panel will consider at every meeting whether any immediate single or multi-agency action is required to respond to emerging issues identified through the review process[3]. They may wish to deliver swift messages to the workforce in specific agencies or disseminate multi-agency learning to a wider workforce. In so doing, the Panel will consider what information is shared and whether this will have an impact on family members or any parallel investigations.
The CSPR Report
Safeguarding Partners are required to publish the learning from all CSPRs. The reviewer will normally draft a report with publication in mined.
Reports should be focused and succinct. They should contain enough information to provide a clear context for the learning and should reflect the perspective of the child and family as well as the views of practitioners. The report should focus on analysis of both practice and system issues and should clearly identify any learning from the review.
Reports should meet any requirements specified in the agreed Terms of Reference for the review and, as a minimum, must include:
- a brief overview of what happened and the key circumstances, background and context of the case. This should be concise but sufficient to understand the context for the learning and recommendations;
- an analysis of any systemic or underlying reasons why actions were taken or not in respect of matters covered by the report
- a summary of why relevant decisions by professionals were taken;
- a critique of how agencies worked together and any shortcomings in this; whether any shortcomings identified are features of practice in general;
- what would need to be done differently to prevent harm occurring to a child in similar circumstances;
- examples of good practice; and,
- a summary of any recommended improvements to be made by persons in the area to safeguard and promote the welfare of children
- what needs to happen to ensure that agencies learn from this case.
Reports should be written in a way that avoids harming the welfare of any children or adults in the case. Information should be appropriately anonymised and very intimate and personal detail of the family’s life should be kept to a minimum to reduce the sensitivity of publication.
The Case Review Panel will be responsible for ensuring the quality of the draft report has met the agreed terms of reference, is succinct and focused on improving local safeguarding arrangements and any proposed recommendations are SMART. The Case Review panel will also pull together a draft action plan
The final report should be formally approved by the Case Review Subgroup followed by the relevant Safeguarding Children Partnership Board.
Publication
The Safeguarding Partners are required to publish the reports of local Child Safeguarding Practice Reviews, unless they consider it inappropriate to do so.[4]
Publication and media planning will commence once the final report (including the agreed recommendations) has been formally endorsed by the Safeguarding Children Partnerships. Publication planning will include strategic leads from the agencies involved in the review and their media/communication leads.
Consideration will be given to how best to manage the impact of the publication on children, family members, practitioners and others closely affected by the case.
The arrangements for informing practitioners will also be considered. The senior managers from each agency will take responsibility for informing frontline staff of the date of publication and ensuring they have appropriate support.
A central point of contact for media enquiries should be identified. This individual can co-ordinate media enquiries during the publication phase and ensure effective liaison is maintained with each organisation’s strategic and press leads.
The Safeguarding Partners must send a copy of the full report to the National Panel, Ofsted and to the Secretary of State no later than seven working days before the date of publication. Reports should be submitted electronically to:
Mailbox.NationalReviewPanel@education.gov.uk
Published reports will always include the name of the reviewer(s) and will be made available to read and download from the Cambridgeshire and Peterborough Safeguarding Partnership Board website. Reports will be publicly available for at least one year and archived reports will be available on request from the Safeguarding Partners.
Published reports will also be submitted for inclusion in the NSPCC National Repository of safeguarding case reviews. Reports will be submitted by email to: information@nspcc.org.uk
CSPR Referral Process Flowchart
Embedding the Learning
The purpose of Rapid Reviews and Local Child Safeguarding Practice Reviews is to identify improvements that can be made to safeguard and promote the welfare of children. Disseminating and embedding the learning is, therefore, crucial.
Capturing improvement and taking corrective action while the review is in progress
Every effort should also be made, both before the review and while it is in progress, to:
|
Working Together to Safeguard Children (2023, Page 141 Paragraph 366)
The CSPR panel will consider at every panel meeting during the review whether any immediate single or multi-agency action is required to respond to emerging issues identified through the review process. They may wish to deliver swift messages to the workforce within specific agencies or disseminate multi-agency learning to a wider workforce. In so doing, the Panel will consider what information is shared and whether this will have an impact on family members or any parallel investigations.
Disseminating and Sharing Learning from the Review
Upon conclusion of the review, a clear plan for disseminating and sharing the learning from with all relevant agencies will be developed. This may include organising single or multi-agency workshops, producing a 7-minute briefing or a set of standard PowerPoint slides on the lessons learned for use within team meetings and/or supervision sessions will be circulated across the partnership.
It is the responsibility of both the CSPR panel and CSPR subgroup members to ensure these are shared internally within their agency as appropriate.
It is the responsibility of agencies who have participated in the review to ensure their agency recommendations are fully implemented and used to make improvements to their safeguarding children arrangements.
The findings from Rapid Reviews and CSPRs including actions taken, progress made, and assurance gained that improvements have positively impacted upon outcomes for children will be included within the Safeguarding Children Partnership’s Annual Report.
Monitoring Progress
The Case Review subgroup will regularly monitor progress on the implementation of recommended improvements, and will follow up actions to ensure improvement is sustained. The impact of the improvement will reported to the Safeguarding Children Partnership
Taking into Account Learning from National Reviews
The relevant Child Safeguarding Practice Review Group will also review the learning from all national reviews and consider how the recommendations can be implemented locally.
Appendix 1 –Referral Form
Appendix 2 – Overview of Parallel Reviews
Effective local liaison is required between Multi-Agency Safeguarding Arrangements, Adult Safeguarding Partnership Boards, Community Safety Partnerships and Multi-Agency Public Protection Arrangements to determine the most appropriate review process to maximise learning and minimise duplication of effort and reduce anxiety for families involved.
Reviews Following the Death of an Adult or Child in England
The following summarises statutory and discretionary reviews that may be undertaken in England following the death of an adult or child. It includes the review name, legal basis, criteria for when the review should be undertaken, who it applies to, and its purpose.
Statutory Reviews
Review Name | Legal Basis | Criteria for Review | Applies To | Purpose |
Child Death Review (CDR) | Children Act 2004 | All deaths of children under 18, excluding stillbirths | Children under 18 | Understand circumstances, identify modifiable factors, improve child health and safety |
Domestic Abuse Related Death Reviews (DARDR) previously known as Domestic Homicide Reviews (DHR) | Domestic Violence, Crime and Victims Act 2004 | Death of a person aged 16+ due to violence, abuse or neglect by a person to whom they were related, with or was in an intimate personal relationship or a member of the same household | Adults (16+) | Learn lessons to prevent future domestic abuse-related deaths |
Safeguarding Adult Review (SAR) | Care Act 2014 | Death or serious harm of an adult with care and support needs due to abuse or neglect | Adults with needs for care and support | Identify lessons to improve safeguarding practice and inter-agency working |
Child Safeguarding Practice Review | Children Act 2004 | Death or serious harm of a child due to abuse or neglect, or where learning can improve safeguarding | Children | Identify lessons to improve safeguarding practice and inter-agency working |
Coroner’s Inquest | Coroners and Justice Act 2009 | Deaths that are violent, unnatural, sudden with unknown cause, or in state detention | All individuals | Determine cause of death and circumstances |
Offensive Weapons Homicide Review* *Currently in pilot stage | Police, Crime, Sentencing and Courts Act 2022 | Homicide involving offensive weapons where the victim is aged 18+ | Adults (18+) | Prevent future serious violence and homicide |
Discretionary or Policy-Driven Reviews
Review Name | Legal Basis | Criteria for Review | Applies To | Purpose |
LeDeR (Learning Disabilities Mortality Review) | NHS England policy | Death of a person with a learning disability | Adults and children | Identify care improvements and reduce inequalities |
Mental Health Homicide Review | NHS England policy | Homicide committed by someone known to mental health services | All individuals | Improve mental health care and risk management |
Death of a Homeless Person Review | Local safeguarding guidance | Death of a person who was homeless or rough sleeping | Adults | Identify systemic failings and improve multi-agency responses |
Drug and Alcohol-Related Death Review | Local authority/public health | Death due to substance misuse, especially if known to services | All individuals | Improve prevention and treatment strategies |
Death in Custody Review | IOPC / PPO | Death in police, prison, or immigration detention | All individuals | Ensure accountability and improve custodial care |
NHS Serious Incident Review / Independent Investigation | NHS England Serious Incident Framework | Death in NHS care where there are concerns about service delivery | All individuals | Ensure transparency, learning, and accountability |
Appendix 3 – Methodology Options
The process for undertaking Case Reviews should be determined locally according to the specific circumstances of individual cases. The most appropriate methodology will normally be that which provides the best opportunity to learn; however, it will be determined by, and be proportionate to, the specific circumstances and the scale of the situation.
Examples of different types of methodologies include:
Traditional Review Model This model is traditionally used where there are demonstrably serious concerns about the conduct of several agencies or inter-agency working and the case is likely to highlight national lessons about safeguarding practice. This model includes
| |
The benefits of this model are:
| The drawbacks of this model are:
It does not always facilitate frontline practitioner input. |
Appreciative Inquiry Case reviews conducted as an appreciative inquiry seek to create a safe, respectful and comfortable environment in which people look together at the interventions that have successfully safeguarded a child; and share honestly about the things they got wrong and/or did not have the desired outcome. They get to look at where, how and why events took place and use their collective hindsight wisdom to design practice improvements. To undertake a case review using the Appreciative Inquiry principles, the facilitator should be familiar with AI and confident in putting this into practice. Appreciative Inquiry is facilitated through the use of strengthen based, solution focused language. Appreciative Inquiry can be used within any methodology of case review. | |
Benefits of this model are:
| Drawbacks of this model are:
|
Reflective Learning Session or Multi- Agency Practitioner Events Where an independent review is not required, information is gathered from agencies to contribute to a reflective learning session, attended by the relevant professionals to critically appraise the case and learning recommendations agreed. | |
Benefits of this model are:
| Drawbacks of this model are:
|
Individual Agency Review This model would be relevant when a serious incident identifies single agency involvement or where potential one agency learning has been identified. There are no implications or concerns regarding involvement of other agencies and it is appropriate that lessons are learnt regarding the conduct of an agency. Such reviews could be requested by the Safeguarding Partnership. If undertaken individually by an agency, the agency concerned should inform the Partnership they are undertaking an Individual Agency Review with a safeguarding element, in order for the Partnership to consider any transferable learning across the partnership. | |
The benefits of this model are:
| The drawbacks of this model are:
|
Multi-Agency Audits Multi-agency audits of case files that relate to a specific theme is an effective mechanism of understanding practice at child level and practitioners and their managers are involved in identifying what they are doing well and where improvements need to be made. A rolling programme of multi-agency audits themes is identified through local priorities, local reviews, inspection findings, performance data and national research. | |
Benefits of this model are:
| Drawbacks of this model are:
|
Peer Review Approach A peer review approach encompasses a review by one or more people who know the area of business and accords with self-regulation and sector led improvement programme. Peer review methods are used to maintain standards of quality, improve performance and provide credibility. They provide an opportunity for an objective overview of practice, with potential for alternative approaches and/or recommendations for improved practice. There are two main models for peer review:
| |
The benefits of this model are:
| The drawbacks of this model are:
Potential to perceive peer reviews from members of the partnership as not sufficiently independent, especially when they concern political or high-profile cases. |
Root Cause Analysis (RCA) Root Cause Analysis (RCA) is an investigation methodology used to understand why an incident has occurred. RCA provides a way of looking at incidents to understand the causes of why things go wrong. If the contributory factors and causal factors – the root causes – of an incident or outcome are understood, corrective measures can be put in place. By directing corrective measures at the root cause of a problem (and not just at the symptom of the problem) it is believed that the likelihood of the problem reoccurring will be reduced. This approach can help to prevent unwanted incidents and outcomes, and also improve the quality and safety of services that are provided. The RCA investigation process can help an organisation, or organisations, to develop and open culture where staff can feel supported to report mistakes and problems in the knowledge this will lead to positive change, not blame. General principles of Root Cause Analysis:
To be effective, the root cause analysis & investigation must establish ALL causal relationships between the root cause(s) and the incident, not just the obvious. | |
The benefits of this model are:
| The drawbacks of this model are:
|
Appendix 4 – Media strategy for response to serious incidents led by Safeguarding Board
In the event of a serious incident or publication of a Child Safeguarding Practice Review or Safeguarding Adults Review; the Safeguarding Partnership Board will have a single initial point of contact for the media which will be the Communications Team at the Local Authority.
Members of the Board should only talk to the media after having first cleared this with the local authority’s Communications Team.
Anyone speaking on behalf of the Safeguarding Partnership Board must ensure that the media knows who they are representing.
Public and media interest
It is the responsibility of designated senior managers in each agency, alongside the Chair of the Safeguarding Partnership Board, to anticipate public and media interest in the death or serious injury of a child or adult at risk, or in the investigation of organised abuse under the umbrella of the Safeguarding Partnership’s safeguarding procedures.
The chair, together with the designated senior managers in liaison with their press offices, must consult to formulate and agree a strategy for managing public information and make the necessary and timely arrangements for any media activity. When agreeing a strategy for managing public information consideration must be given to the following:
- The need to maintain confidentiality in respect of personal information contained within reports on the child, family members and others;
- The accountability of public services and the importance of maintaining public confidence in the process of internal review;
- The need to secure full and open participation from the different agencies and professionals involved;
- The responsibility to provide relevant information to those with a legitimate interest;
- The constraints on sharing information when criminal proceedings are outstanding, in that access to the contents of information may not be within the control of Safeguarding Partnership Board.
- It is the duty of senior managers to ensure that all staff undertaking enquiries are aware of the agreed strategy and response to approaches by the public and media representatives, and are enabled to proceed with their work without excessive public pressure and exposure.
Specific media enquiries
A dialogue with key contacts will be established to determine which organisation will take lead responsibility for responding to media enquiries relating to any specific event. This initial dialogue will establish which matters, if any, will be handled collectively by the safeguarding partners and which will be handled by individual board partners. A decision will also be made whether to publish a proactive statement or reactive statement on behalf of the safeguarding partnership.
Ongoing responsibility for co-ordinating this activity will remain with the local authority Communications Team, except where the key contacts agree that the press office of another board partner will take the lead in a particular case. The Head of Service for the Cambridgeshire and Safeguarding Partnership Board will be kept informed of all actions undertaken and will be sent a copy of all communication with the media for inclusion in the audit trail.
Appendix 5 – Media Alert In Relation To a Serious Incident Involving a Child or Young Person
In the event of a media alert in relation to a serious incident involving a child or young person, the media lead of the partner organisation receiving the information should alert the Local Authority’s Communications Team
The local authority’s Communications Team will then alert the Chair of the Safeguarding Board and communications leads for all relevant partner agencies.
All communications leads to inform operation lead in their own agency.
A meeting of the key media leads will be convened as soon as possible. If this is not possible, media responses will be approved with the Safeguarding Board Chair and the media leads of the key organisations.
[1] by the Child Safeguarding Practice Review and Relevant Agency (England) Regulations 2018.
[2] For example, Domestic Homicide Reviews, multi-agency public protection arrangement reviews, Safeguarding Adult Reviews or health ‘serious untoward incident’ processes.
[3] This ensures compliance with Working Together 2018 which requires that ‘every effort should be made, both before the review and while it is in progress to (i) capture points from the case about improvements needed, and (ii) take correction action and disseminate learning.’
[4] If they consider it inappropriate to publish the report, they must publish any information about the improvements that could be made following the review.