Issue No: | 1 |
Document Owner: | Cambridgeshire Safeguarding Children Partnership Peterborough Safeguarding Children Partnership |
Date Approved: | |
Date Published: | 23 January 2026 |
Review Date: |
Table of Contents
1. Background and purpose of this guidance
This local practice guide has been developed to raise awareness about FGM in Peterborough and Cambridgeshire amongst practitioners. It attempts to summarise the issues for identifying, responding and preventing FGM for both children and adults. These are practice guidelines and are designed to be educative and provide advice; they are not a substitute for existing statutory guidance such as Working Together to Safeguard Children (2023).
Please note the below guidance refers to ‘patients’ which covers all children and adult females who may have contact with safeguarding services. Cambridgeshire and Peterborough Safeguarding Children’s Partnerships endorse the use of this guidance by all agencies in the management of FGM.
2. What we know about FGM
What is FGM?
FGM includes any mutilation of a female’s genitals, including the partial or total removal of the external genitalia for perceived cultural or other non-medical reasons (Please see Appendix one for further details). The practice is medically unnecessary, extremely painful and has serious health consequences, both at the time when the mutilation is carried out and in later life. It was made illegal in the UK in 1985; the most recent laws covering this area is the Female Genital Mutilation Act 2003 and amendments within the Serious Crime Act 2015.
Who is at risk?
The World Health Organisation estimates that three million girls undergo some form of the procedure every year in Africa alone. It is practised in 28 countries in Africa and some in the Middle East and Asia. FGM is also found in the UK amongst members of migrant communities. It is estimated that approximately 60,000 girls aged 0-14 were born in England and Wales to mothers who had undergone FGM. UK communities that are most at risk of FGM include Kenyan, Somali, Sudanese, Sierra Leonean, Egyptian, Nigerian and Eritrean. Non-African communities that practise FGM include Yemeni, Afghani, Kurdish, Indonesian and Pakistani.
FGM can be practised at any age. People from some communities within certain countries are more likely to practise FGM than others; this does not mean that every community from a particular country does practise FGM. Prevalence rates and research on FGM in specific countries across the world can be accessed via the National FGM Centre’s interactive map .
Girls may be at increased risk of harm if their mother, or any sisters / female members of the extended family, have experienced FGM. FGM is practised by families for a variety of complex reasons but usually in the belief that it is beneficial for the girl or woman.
Talking about FGM
FGM is a complex and sensitive issue that requires professionals to approach the subject carefully. When talking about FGM, professionals should:
- make no assumptions.
- give the individual time to talk and be willing to listen.
- create an opportunity for the individual to disclose, seeing the individual on their own in private.
- be sensitive to the intimate nature of the subject.
- be non-judgemental (pointing out the illegality and health risks of the practice but not blaming the girl or woman).
- get accurate information about the urgency of the situation if the individual is at risk of being subjected to the procedure.
- take detailed notes.
- use simple language and ask straightforward questions.
- use terminology that the individual will understand.
- avoid loaded or offensive terminology such as ‘mutilation’
- use value-neutral terms understandable to the woman, such as:
- “Have you been closed?”
- “Were you circumcised?”
- “Have you been cut down there?”
- give the message that the individual can come back to you if they wish.
- give a clear explanation that FGM is illegal and that the law can be used to help the family avoid FGM if/when they have daughters.
An accredited female interpreter may be required. Any interpreter should not be a family member and not be known to the individual. This is because girls or women may feel embarrassed to discuss sensitive issues in front of such people and there is a risk that personal information may be passed on to others in their community and place them in danger.
The department of health has created 3 risk assessments templates that can be used during a conversation with a victim of FGM who is: pregnant/or recently given birth, non-pregnant adult over 18, or a child/young adult under the age of 18. Using the templates can assist a professional to decide as to whether an individual is at risk of harm from FGM. Please see FGM Professional Guidance Forms.
3. Identifying girls and women at risk
Specific factors that may heighten a girl’s or woman’s risk of being affected by FGM
There are several factors in addition to a girl’s or woman’s community that could increase the risk that she will be subjected to FGM:
- The level of integration within UK society – it is believed that communities less integrated into British society are more likely to carry out FGM.
- Any girl born to a woman who has been subjected to FGM must be considered at risk, as well as other female children in the extended family.
- Any girl who has a sister who has already undergone FGM must be considered at risk, as must other female children in the extended family.
- Any girl withdrawn from personal, social and health education may be at risk because of her parents wishing to keep her uninformed about her body and rights.
Indications that FGM may be about to take place soon
The age at which girls undergo FGM varies enormously according to the community. The procedure may be carried out when the girl is newborn, during childhood or adolescence, at marriage or during the first pregnancy. However, many cases of FGM are thought to take place between the ages of 5 and 8 and therefore girls within that age bracket are at a higher risk.
It is believed that FGM happens to girls in the UK as well as overseas (often in the family’s country of origin). Girls of school age who are subjected to FGM overseas are thought to be taken abroad at the start of the school holidays, particularly in the summer holidays, for there to be sufficient time for her to recover before returning to her studies.
There can also be clearer signs when FGM is imminent:
- It may be possible that families will practise FGM in the UK when a female family elder is around, particularly when she is visiting from a country of origin.
- A professional may hear reference to FGM in conversation, for example a girl may tell other children about it.
- A girl may confide that she is to have a ‘special procedure’ or to attend a special occasion to ‘become a woman’.
- A girl may request help from a teacher or another adult if she is aware or suspects that she is at immediate risk.
- Parents state that they or a relative will take the child out of the country for a prolonged period.
- A girl may talk about a long holiday to her country of origin or another country where the practice is prevalent.
Indications that FGM may have already taken place:
There are several indications that a girl or woman has already been subjected to FGM:
- A girl or woman may have difficulty walking, sitting or standing.
- A girl or woman may spend longer than normal in the bathroom or toilet due to difficulties urinating.
- A girl may spend long periods of time away from a classroom during the day with bladder or menstrual problems.
- There may be prolonged or repeated absences from school or college.
- A prolonged absence from school or college with noticeable behaviour changes (e.g. withdrawal or depression) on the girl’s return could be an indication that a girl has recently undergone FGM.
- A girl or woman may be particularly reluctant to undergo normal medical examinations.
- A girl or woman may ask for help, but may not be explicit about the problem due to embarrassment or fear.
4. The law and the need to safeguard girls and young women at risk of FGM
Under section 47 of the Children Act 1989, anyone who has information that a child is potentially or actually at risk of significant harm is required to inform social care or the police. A local authority should exercise its powers to make enquiries to safeguard a girl’s welfare under section 47 if it has reason to believe that a girl is likely to be subjected to or has been subjected to FGM. Where a girl appears to be in immediate danger of FGM, consideration should be given to legal interventions.
The Female Genital Mutilation Act 2003 makes it illegal to
- practice FGM in the UK
- take girls who are British nationals or permanent residents of the UK abroad for FGM.
- aid, abet, counsel, or procure the carrying out of FGM abroad.
- help a girl perform FGM on themselves in or outside the UK.
- help a girl perform FGM on themselves in or outside the UK.
Any person found guilty of an offence under the Act will be liable to a maximum penalty of 14 years imprisonment or/and a fine.
Section 70-75 of the Serious Crime Act 2015 extended the scope of extra territorial offences, granted victims of FGM life- long anonymity and introduced a new offence of failing to protect a girl from the risk of FGM. These provisions introduced FGM Protection Orders and a mandatory duty for front line professionals to report FGM.
Female Genital Mutilation Act 2003
Section 1 – A person is guilty of an offence if he/she excises, infibulates or otherwise mutilates the whole or any part of a girl’s labia majora, labia minora or clitoris.
Section 2 – A person is guilty of an offence if he/she aids, abets, counsels or procures a girl to carry out FGM on herself
Section 3 – Makes it an offence for a person in the UK to aid, abet, counsel or procure the performance outside the UK of FGM that is carried out by a person who is not a UK National or permanent resident. So the person who, for example, arranges by telephone from England for his UK national daughter to have FGM carried out abroad by a foreign national (who does not live permanently in the UK) commits an offence.
Section 4 – Extends sections 1, 2 and 3 of the Act so that any of the prohibited acts done outside the UK by a UK national or permanent UK resident will be an offence under UK law and triable in the courts of England, Wales and Northern Ireland. (Scotland has separate legislation – the Prohibition of Female Genital Mutilation (Scotland) Act 2005.)
By virtue of section 8 of the Accessories and Abettors Act, it is also an offence for:
- a person in the UK; or
- a UK national or permanent UK resident outside the UK
To aid, abet, counsel or procure a UK national or permanent UK resident to carry out FGM outside the UK. For example, if a person in the UK advises his UK national brother over the telephone how to carry out FGM abroad, he is guilty of an offence.
The effects of the extension of section 2 is that it is an offence for a UK national or permanent UK resident outside the UK to aid, abet, counsel or procure a person of any nationality to carry out FGM on herself wherever it is carried out.
The effect of the extension of section 3 is that it is an offence for a UK national or permanent UK resident outside the UK to aid, abet, counsel or procure a foreign national (who is not a permanent UK resident) to carry out FGM outside the UK on a UK national or permanent UK resident. For example, a permanent UK resident who takes his permanent UK resident daughter to the doctor’s surgery in another country so that FGM can be carried out, is guilty of offence.
Female Genital Mutilation Protection Orders
Are granted by the courts and offer a legal means to protect and safeguard victims and potential victims of FGM. This could include, for example, surrendering a passport to prevent a person at risk being taken abroad for FGM. They can be applied for by:
- the person who has had or is at risk of FGM
- a local authority
- any other person with the permission of the court (for example, the police, a teacher, a charity or a family member).
Further details can be found at: FGMPO Factsheet
Duty to notify the police of FGM (mandatory reporting):
This section places a duty on those who work in ‘regulated professions’ namely healthcare professionals, teachers, and social care workers, to notify the police when, in the course of their work, they discover that an act of FGM appears to have been or is going to be carried out on a girl who is under 18. Failing to comply with the duty will be dealt with via existing disciplinary measures, which may include referral to the professional regulator and/or Disclosure and Barring Service as appropriate. It is important to be aware of other children in the household as there could be transient risks such as the potential for them to also be at risk of undergoing FGM or being exposed to harmful practices.
5. Individual agency responsibilities
All professionals should be familiar with the risk indicators of FGM and be aware of what steps to take if they are concerned that a child/ young person has or is likely to be the victim of FGM. Remember reporting FGM is a mandatory legal duty.
Female Genital Mutilation Information System (FGM-IS)
Is a live IT system launched by the DOH and NHS England and has been active since 2015 to support efforts to eliminate FGM worldwide. At the point of a family history of FGM being identified for a female infant, an FGM-IS alert should be added by authorised professionals or administrative staff to the child’s National Care Record. Ideally this should be completed at birth. This allows authorised care professionals throughout England to be alerted to the family having a history of FGM when the child presents to a healthcare setting and the national care record is checked.
Appendix 1 – World Health Organisation (WHO) FGM Classification
Female genital mutilation is classified into four major types. The World Health Organisation defines FGM as follows:
- Type 1: Clitoridectomy: partial or total removal of the clitoris (a small, sensitive and erectile part of the female genitals) and, in very rare cases, only the prepuce (the fold of skin surrounding the clitoris).
- Type 2: Excision: partial or total removal of the clitoris and the labia minora, with or without excision of the labia majora (the labia are “the lips” that surround the vagina).
- Type 3: Infibulation: narrowing of the vaginal opening through the creation of a covering seal. The seal is formed by cutting and repositioning the inner, or outer, labia, with or without removal of the clitoris.
- Type 4: Other: all other harmful procedures to the female genitalia for non-medical purposes, e.g. pricking, piercing, incising, scraping and cauterizing the genital area.
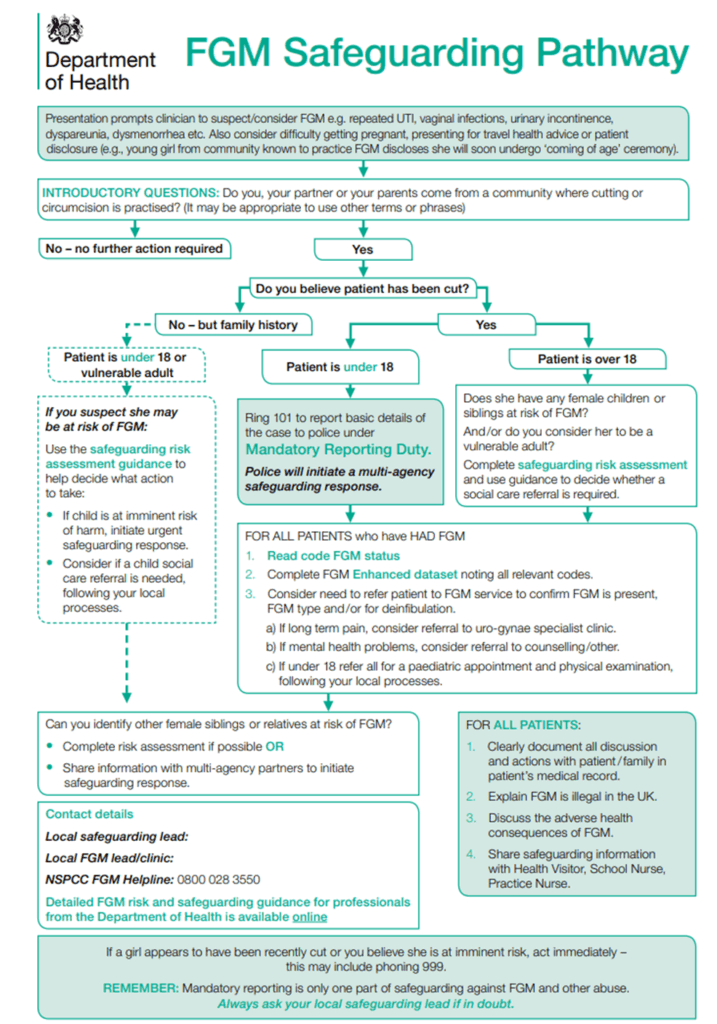
Appendix 2 FGM Safeguarding Pathway
Appendix 3 FGM Mandatory Reporting Poster

Appendix 4 FGM Mandatory Reporting – What you need to do